Feeling dizzy when all your medical tests are normal, can be confusing and frustrating. This is common in Persistent Postural-Perceptual Dizziness (PPPD) also known as Triple PD.
PPPD is real and treatable. With consistent vestibular rehabilitation therapy (VRT), cognitive behavior therapy (CBT), and gradual exposure, most people see gradual improvement.
In this blog, we’ll explore what Persistent Postural-Perceptual Dizziness (PPPD) is, its symptoms, causes, diagnosis, and how ENT specialists treat it.
What is Persistent Postural-Perceptual Dizziness (PPPD)?
Persistent Postural-Perceptual Dizziness, or PPPD, is a chronic functional condition characterized by long-lasting dizziness, unsteadiness, and motion sensitivity.
Unlike brief episodes of vertigo, PPPD symptoms persist for three months or more. It worsens in situations like:
Standing for long periods or walking
Busy or crowded places
Watching moving visuals- scrolling screens
Doctors describe PPPD as a functional disorder. This does not mean the symptoms are imaginary or “just in the mind.” Functional simply means that the structure of the inner ear and brain is intact, but the function is disrupted.
It involves a dysregulation of the brain’s balance and sensory processing systems.
After an initial vestibular insult (like a previous vertigo attack, inner ear infection, or migraine-related vertigo), the brain gets stuck in a “hyper-alert” mode and maladapt, leading to persistent perception of movement or imbalance even when the body is still.
Think of it as having perfectly working “hardware” but a misfiring “software program.
Though tests such as MRI scans, VNG or audiometry may appear normal, the dizziness is genuine and can interfere with work, travel, and social life.
Proper vestibular and cognitive therapy can lead to significant improvement.
Symptoms of Persistent Postural-Perceptual Dizziness (PPPD)
PPPD symptoms follow a distinct pattern. Instead of sudden spinning vertigo attacks, PPPD usually causes a more persistent, chronic imbalance and ongoing dizziness that interferes with daily life.
Common PPPD Symptoms
Persistent unsteadiness or lightheadedness: Feeling as if you are swaying, rocking, or floating even when standing still.
Motion sensitivity: Dizziness worsens with motion like when walking, turning your head, or being in moving environments such as traffic, escalators, or crowds.
Visual triggers: Busy visual patterns, scrolling screens, or watching moving objects can intensify dizziness symptoms. Anxiety or discomfort in visually busy environments (shopping malls or crowded streets)
Heightened anxiety or discomfort: Brain goes in constant threat mode. Due to heightened anxiety and fear of falling people tend to avoid certain places or situation this in turn leads to dizziness-fear-dizziness loop.
Mild nausea: Some patients report queasiness, especially in visually stimulating environments.
Key Points to Understand About PPPD Symptoms:
Duration: Symptoms usually last for three months or more, which separates PPPD from short-lived vertigo conditions.
Trigger-specific: PPPD is not constant every moment it tends to worsen with posture changes, motion, or visually busy environments.
Follows other vertigo /dizziness conditions: PPPD often develop after vestibular migraine, Ménière’s disease, concussion, or inner ear infections.
Evaluation by an ENT or vertigo specialist is important for proper diagnosis of PPPD.
Keeping a symptom diary, noting when dizziness worsens, what triggers it, and how long it lasts, can be very helpful for your doctor to distinguish PPPD from other vestibular disorders
Persistent Postural-Perceptual Dizziness often begins after an initial vertigo attack. Understanding these causes helps both patients and doctors create a treatment plan.
Common Causes of PPPD: The Brain-Ear Disconnect
Previous Vestibular or Neurological Dizziness: Vestibular migraine, Ménière’s disease, or vestibular neuritis can trigger PPPD. Even after you recover from your original vertigo attack, your brain may continue to misinterpret balance signals. This may lead to persistent dizziness.
Sensory Processing Changes: PPPD is partly a brain-processing issue. The brain “overcompensates” for balance signals, creating a mismatch between what your eyes, inner ear (vestibular), and body feel.
This mismatch of sensory information by your nervous system may cause constant functional dizziness.
Psychological Stress or Anxiety: Stress, fatigue, or heightened anxiety can amplify the perception of imbalance and dizziness.
Threat or hyper alert mode– Brain goes in hyper alert mode. Causing mal adaptive behaviors such as stiff posture, overanalyzing motion and avoiding certain situation due to fear of dizziness. This avoidance further delays natural compensation of brains balance system.
Common Triggers That Worsen PPPD
Many people with Persistent Postural-Perceptual Dizziness notice that certain situations can worsen the sensation of imbalance.
Standing for long periods or walking on soft or uneven surfaces – Patients often describe it as “like trying to balance on a mattress that won’t stay still.
Busy or crowded places– shopping malls, traffic, office corridors, or even a family gathering where multiple people are moving around, can overwhelm the brain’s balance system.
Motion and visual flow- escalators, elevators, car rides, or even scrolling on a phone or computer screen, may worsen the sense of swaying or floating. Some patients say it feels “like being on a boat in choppy water.”
Life style: Fatigue, poor sleep, or emotional stress can lower the brain’s ability to compensate, making functional dizziness symptoms more noticeable.
How PPPD Develops?
PPPD usually begins after a triggering vestibular event such as a BPPV, Menieres disease, vestibular migraine, or an inner ear infection. Although the initial condition may settle, the balance system doesn’t always “reset”.
Brain overreacts to this vertigo attack. It begins to lean on visual cues (what the eyes see) and postural cues (how the body feels while standing or walking) rather than inner ear vestibular signals.
This creates a mismatch. This information such as scrolling screens, busy traffic, crowds, sends confusing threat signals to the brain.
As a result patients feel persistent dizziness, swaying, or unsteadiness, even though their ears and neurological exams may appear normal.
This explains why PPPD symptoms are not purely “in the ear” but also involve how the brain processes balance.
That’s why treatment often combines vestibular rehabilitation with behavioral or psychological support, rather than relying on medicines alone.
Diagnosis of Persistent Postural-Perceptual Dizziness
There isn’t a single scan or blood test that confirms Persistent Postural-Perceptual Dizziness. Diagnosis of PPPD is a careful process of listening to the patient’s dizziness symptoms, ruling out other disorders, and using targeted balance tests.
Because symptoms often overlap with conditions like vestibular migraine, Ménière’s disease or anxiety-related dizziness, the experience of an ENT specialist becomes very important in reaching the right diagnosis.
How ENT Specialists Diagnose PPPD?
Detailed History of Symptoms
ENT specialist spend time on the details such as when the dizziness started, Duration of symptoms (PPPD usually persists for three months or more), What specific situations make it worse, for example, standing for a long time, walking in a crowd, moving cars or scrolling on your phone.
We’ll also ask about past vertigo attacks, vestibular migraines, head injury, or ear infections, and about sleep, medications and stress. A short symptom diary (what you were doing when it got worse, how long it lasted) is one of the most helpful things you can bring.
Often the history of symptoms gives the clearest hint that we’re dealing with PPPD because it is a functional dizziness disorder, where the balance system is intact and all tests may come normal.
Vestibular Tests to Check the Balance System
If your history suggests PPPD or another vestibular problem, we may do tests to assess your balance system, common balance tests include:
VNG (Video Nystagmography): VNG helps us spot abnormal eye movements or nystagmus linked to the balance organs.
VEMP (Vestibular Evoked Myogenic Potential): Measure reflex activity between the inner ear and neck/eye muscles to check parts of the vestibular nerve.
Posturography: You stand on a platform and we test how you keep balance under different visual or surface conditions. It shows whether you rely too much on vision or have trouble using other balance cues. In PPPD these tests are often normal, or they show a pattern of visual dependence; either way they’re useful to rule out other causes of vertigo or dizziness and to plan the right rehabilitation exercises.
Ruling out other dizziness conditions
Audiometry (a simple hearing test) is used to look for the hearing changes seen in Ménière’s disease. MRI is reserved for cases with red flags for example, significant asymmetric hearing loss or neurological signs to exclude structural or central issues.
Not everyone needs every test; we choose investigations that will actually change the diagnosis or treatment plan
Symptom questionnaires
Sometimes the most valuable test isn’t a machine, but what you actually experience.
You may be asked to fill out standardized questionnaires that measure how often dizziness occurs, how severe it feels, and what makes it worse.
These tools help us diagnose whether your pattern matches functional dizziness like PPPD, or whether it fits an episodic vestibular disorder such as vestibular migraine.
Anxiety and function assessment questionnaires like GAD7, HADS, and Dizziness Handicap inventory (DHI) helps in initial assessment and post treatment outcome.
The Bárány Society Criteria (2017) for Diagnosis of PPPD
According to the Bárány Society, PPPD is diagnosed when dizziness lasts most days for at least three months,worsens with standing, walking, or visually busy places, begins after a vestibular event like vertigo or migraine, and isn’t explained by another disorder.
The Bárány Society, an international vestibular research group, has set clear diagnostic guidelines for PPPD. According to their criteria, PPPD is diagnosed when:
Dizziness, unsteadiness, or non-spinning vertigo is present on most days for ≥3 months
Symptoms worsen with upright posture, active or passive motion, or exposure to complex visual stimuli
The disorder is precipitated by a vestibular event, neurological condition, or psychological distress
No other condition explains the symptoms better
These criteria provide a reliable framework, ensuring that PPPD is recognized as a distinct condition not “all in the head,” but a real, functional disorder.
Treatment Options for Persistent Postural-Perceptual Dizziness (PPPD)
Persistent Postural-Perceptual Dizziness is treatable. With a combination of vestibular rehabilitation, behavioural therapy, and lifestyle adjustments, most patients can regain balance, confidence, and daily functioning.
Treatment of PPPD is always tailored to the individual.
Vestibular Rehabilitation Therapy (VRT) for PPPD Recovery
Vestibular Rehabilitation Therapy is a cornerstone of PPPD treatment. These are specialized balance and eye–head coordination exercises to retrain your brain how to process motion and spatial information correctly.
Patients usually start with exercises for gaze stabilization (training your eyes to move smoothly while your head moves) and balance control.
Patients are gradually exposed to real-life situations and everyday triggers like walking in a busy street, turning quickly, or navigating visually complex environments in a safe graded way. (Starting with simple situation and gradually progressing to more complex ones.)
Even a few minutes of consistent home practice can bring visible improvement within weeks.
Cognitive Behavioral Therapy (CBT) for PPPD
Many patients with PPPD develop anxiety, fear of falling, or constant worry about when the next dizzy spell might come.
As we know PPPD develops due to maladaptive behavior where patients start avoiding situations which make them dizzy. This leads to a cycle – “dizziness –> fear –> avoidance –> more dizziness.”
Cognitive behavioural therapy (CBT)helps break this loop. Through guided CBT sessions, patients learn to reframe negative thoughts, and calm the over-alert balance system.
Lifestyle and Gradual Exposure in PPPD
Lifestyle adjustments can support recovery from PPPD, such as-
A good Sleep – It helps brain cope better
Relaxation – Yoga, mindfulness, meditation, or breathing exercises reduce the body’s sensitivity to triggers.
Facing triggers slowly: Instead of avoiding crowded markets or bright screens altogether, specialists often recommend gradual reintroduction in a step-by-step way.
Screen time: Cutting down on screen time ease strain.
These daily tips are not a replacement of PPPD management but along with CBT and VRT it helps in early recovery.
Anti-Anxiety Medications
Most patients improve without long-term medicines. However, doctors may prescribe short courses of anti-anxiety drugs such as SSRI and SNRI to reduce the associated anxiety and intensity of dizziness.
These are usually supportive and tapered off once therapy begins to work.
A mix of Vestibular rehabilitation (VRT), Cognitive Behavioural Therapy (CBT), and medical treatment for PPPD, along with gradual exposure helps in management of PPPD.
Living with Persistent Postural-Perceptual Dizziness
Living with PPPD can be tiring. Small everyday things like standing in a queue, walking through a crowded market, or scrolling your phone may feel uncomfortable. It’s natural to feel anxious or low because of this.
But the important thing to remember is: PPPD is treatable, and you can get better with steady care.
Small steps you can take–
Gradual exposure – Gradual exposure to places or situation which makes you dizzy is important part of PPPD treatment.
For example, if you fear crowded shopping malls, start with short visits and over time increase your time there.
Mindful action. It is important to reset the brain from hyperalert mode. Paying attention to your steps or your breath while walking, instead of letting the fear of imbalance take over.
Relaxation techniques– Diaphragmatic breathing, yoga or meditation can help calm the nervous system.
Talk with family: Sharing your experience with family, friends, or even a support group reduces the sense of isolation.
Healthy Routine: Good sleep, stress relief, and reducing screen time support recovery.
Improvement doesn’t happen overnight, its gradual. Consistent vestibular rehabilitation therapy, cognitive behavioural therapy, gradual exposure and anti-anxiety medications (SSRI and SNRI), most PPPD patients gradually recover and regain confidence in their routine activities.
ENT specialist who has experience working with persistent dizziness can adjust treatment step by step.
When to See a Vertigo Specialist for PPPD?
If you’ve been feeling persistent dizziness, unsteadiness, or light-headedness for more than three months, it may be time to consult an ENT specialist.
When everyday activities like walking in a shopping mall or driving in traffic makes you dizzy or uneasy, it may be Persistent Postural-Perceptual Dizziness.
An ENT doctor who understands balance problems can help find out if it’s Persistent Postural-Perceptual Dizziness (PPPD) and guide you toward the right treatment.
Red Flags
Sudden, severe vertigo or imbalance
Sudden hearing loss or ringing in the ears (tinnitus)
Anxiety doesn’t directly cause PPPD, but it can amplify your symptoms and can cause fear-dizziness -fear loop leading to persistent dizziness. CBT to manage anxiety along with gradual exposure is important part of PPPD treatment.
Crowded or visually busy environments (such as shopping malls, traffic).
Active or passive Motion, either you are moving like turning head, walking or surrounding visuals are moving like escalators, moving vehicles, or scrolling screens.
PPPD rarely resolves without targeted treatment. Early treatment, vestibular rehabilitation, and cognitive behavioural therapy help in recovery and reduce chronic dizziness symptoms.
Diagnosing PPPD is a clinical judgement of an ENT specialist, which comes with experience.
Vestibular tests usually come normal, but are advised to rule out other inner ear or neurological causes of chronic dizziness. Following tests are usually recommended-
To diagnose PPPD, ENT specialists use Bárány Society criteria to confirm that symptoms fit PPPD. Symptom questionnaires and vestibular tests (VNG) can be used to rule out other conditions causing chronic dizziness such as vestibular migraine, Ménière’s disease, or neurological disorders.
Yes. PPPD or Persistent Perceptive Postural Dizziness can be managed with a combination of vestibular rehabilitation therapy (VRT), Cognitive Behavioral Therapy (CBT) and ant- anxiety medications. Treatment of PPPD is aimed at gradual exposure to dizziness-triggers and improving functions.
Takeaway
Persistent Perceptive Postural Dizziness (PPPD) can significantly affect daily functioning but it is treatable.
Thorough evaluation of symptoms and clinical vestibular tests are usually enough to diagnose; however, it is important to differentiate PPPD from conditions like Ménière’s disease or vestibular migraine, and advanced tests such as VNG, Posturography, VEMP and MRI scans may be needed.
Early treatment by an ENT specialist helps in faster recovery from chronic dizziness.
At our Vashi vertigo clinic, we specialize in managing PPPD with a mix of vestibular rehabilitation, CBT and gradual exposure, helping patients regain balance and confidence.
Hi, I’m Dr. Archana Jhawar, an ENT specialist with over 24 years of experience. I specialize in tinnitus treatment, vertigo , ear care, and ear surgeries, practicing at Neoalta Clinic, Vashi, and Kokilaben Dhirubhai Ambani Hospital in Navi Mumbai. I’ve trained in vertigo management and Rational Emotive Behavior Therapy (REBT), combining science with compassion to offer holistic, evidence-based care. I’m passionate about writing, poetry, music, yoga, and photography.


 Standing for long periods or walking on soft or uneven surfaces – Patients often describe it as “like trying to balance on a mattress that won’t stay still.
Standing for long periods or walking on soft or uneven surfaces – Patients often describe it as “like trying to balance on a mattress that won’t stay still. Patients usually start with exercises for gaze stabilization (training your eyes to move smoothly while your head moves) and balance control.
Patients usually start with exercises for gaze stabilization (training your eyes to move smoothly while your head moves) and balance control.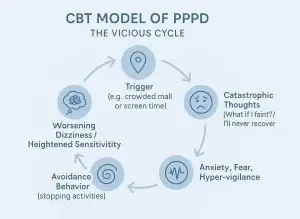 As we know PPPD develops due to maladaptive behavior where patients start avoiding situations which make them dizzy. This leads to a cycle – “dizziness –> fear –> avoidance –> more dizziness.”
As we know PPPD develops due to maladaptive behavior where patients start avoiding situations which make them dizzy. This leads to a cycle – “dizziness –> fear –> avoidance –> more dizziness.”