
A patient came to my clinic in Vashi after four months of antibiotics for a sinus headache. Her nose was clear. Her CT scan was normal. She had migraine, not sinusitis.
It is one of the most consistent patterns in my clinic. Sinusitis and migraine overlap closely enough in symptoms that self-diagnosis is unreliable and treating the wrong condition gives no lasting relief.
This blog helps you understand the difference, what causes persistent headache or facial pain in Navi Mumbai specifically, and when to seek ENT evaluation.

Sinusitis and Migraine both share facial pressure, heaviness around the eyes, and in migraine, even genuine nasal congestion.
Here is a comparison of key features:
| Symptom | True Sinusitis | Migraine |
|---|---|---|
| Nasal discharge | Thick, yellow or green mucus | Clear or no discharge |
| Sense of smell | Often reduced or lost | Usually normal, though strong smells may trigger pain |
| Bending forward | Pain increases significantly over cheeks or forehead | Throbbing may continue but does not shift clearly with position |
| Duration | Days to weeks, worsens without treatment | Episodic attacks, hours to days, then clears |
| Associated signs | Fever, dental pain, or facial swelling | Light sensitivity, sound sensitivity, nausea, or dizziness |
| Response to antibiotics | Bacterial sinusitis may improve | No improvement. Migraine does not respond to antibiotics. |
Diagnosis is made on the pattern of symptoms together, combined with clinical examination.
Migraine directly affects the trigeminal nerve pain pathways, which supply your forehead, eyes, face, and nasal passages.
During an attack, this primary nerve network, known as the trigeminovascular system, becomes highly overactive.
This triggers an autonomic reflex that produces parasympathetic activation of your nasal lining, causing sudden congestion and a watery discharge.
In simple terms: The exact same nerve pathway causing your headache also causes your sinus-like symptoms.
This is why so many patients feel facial pressure, heaviness around the eyes, and a feeling of sinus blockage during a migraine are mistaken for sinusitis.
Many patients have weather-triggered symptoms and blame their sinuses, unaware that sudden weather changes are actually a classic migraine trigger.
Not every headache with facial pressure is sinusitis but certain features make it more likely:
Pain that increases when bending forward: Leaning forward causes worsening of pain or heaviness over the cheeks or forehead that is more typical of sinusitis than migraine.
Thick, coloured nasal discharge: Yellowish or greenish mucus alongside facial pain suggests active bacterial sinus infection.
Reduced or lost sense of smell: Anosmia (loss of smell) occurs when sinus inflammation or nasal polyps block the area of the nose where smell receptors are located. It is an indicator of sinus involvement.
Symptoms that clearly follow a cold or allergy flare: Sinusitis most commonly develops after an upper respiratory infection or during allergy season. If your headaches have no such pattern and come on unpredictably, sinusitis is less likely.
Migraine is frequently underdiagnosed in patients presenting to ENT clinics. Migraine is more likely when you notice one or more of the following:
Throbbing or pulsating quality: A throbbing pain, often on one side of the head, is characteristic of migraine.
Nausea or vomiting during the headache: Nausea accompanying a headache with or without vomiting, is a formal diagnostic criterion for migraine per ICHD-3.
Sensitivity to light or sound: If a headache forces you to lie in a dark, quiet room, migraine is a likely cause.
Sensitivity to light or sound during a headache is a formal diagnostic criterion for migraine per the International Classification of Headache Disorders (ICHD-3) it is rarely seen in sinusitis.
Episodic pattern: Migraine comes in attacks, a period of pain, then a period of no pain.
If your headaches follow this pattern, migraine is worth considering.
Motion sickness or travel sickness: A person or someone in his family having motion sickness or feels nausea during travel or in swings is a recognised migraine-related pattern.
Clear nose despite facial pressure: If your nose feels relatively clear but you still have significant facial pain or pressure, this is more consistent with migraine than sinusitis.
No response to multiple courses of antibiotics. If you have had three or more antibiotic courses for ‘sinus’ pain without improvement, the diagnosis needs to be reconsidered.
Dizziness or a floating sensation alongside the headache: When headache is accompanied by dizziness, imbalance, or a rocking sensation, vestibular migraine should be considered. This is a distinct condition that an ENT specialist is well placed to assess.
When a patient tells me that medicines work for a few days and then the pain returns, the first thing I think about is whether the problem is structural.
Medicines such as antibiotics, nasal sprays, decongestants, reduce infection and inflammation. They cannot change the physical anatomy of the nose.
If a deviated nasal septum is blocking a sinus drainage pathway, or if accumulated fluid or nasal polyps are obstructing airflow, medication may not work.
In chronic sinusitis, repeated inflammation can cause the sinus lining to thicken over time, further narrowing the drainage pathways. When this happens, endoscopic sinus surgery may be needed.
For patients whose sinus symptoms keep returning despite treatment, read blog: “Chronic Sinus Infection: When Medicines Fail and Surgery is considered.“
These patients often experience a pattern of partial improvement followed by relapse when the medication is stopped. And the cycle repeats.
Because Migraine is a neurological issue rather than an infection, antibiotics do nothing for a migraine, and typical nasal sprays and steam inhalation provide temporary comfort. It does not treat the underlying issue.
Living in a coastal city like Navi Mumbai means many patients deal with humidity, changing weather, and year-round allergy exposure causing recurrent sinus conditions.
Humidity and fungal sinus debris:
High humidity, particularly during and after monsoon, can cause fungal-related sinus conditions that do not behave like typical bacterial infections. Symptoms often continue despite repeated antibiotic courses.
Allergy-driven congestion: Nasal allergies cause chronic nose congestion and poor sinus drainage. Symptoms worsen with seasonal changes, dust, and other local triggers.
Structural issues: DNS and nasal polyps: A deviated nasal septum or nasal polyps impair sinus drainage regardless of climate. In Navi Mumbai’s humid environment, this further worsens the symptoms.
Yes. Many patients with migraine-related facial pain have completely normal sinus CT scans because the pain is not coming from blocked sinuses or infection.
However, a normal CT scan does not completely rule out sinusitis, particularly in patients with acute symptoms.
A normal CT does not always explain why you continue to have symptoms. CT findings always need to be interpreted alongside the patient’s history and examination findings
When facial pain, pressure, or headaches persist, ENT clinical examination and nasal endoscopy often help to determine whether the cause is sinus-related or whether another condition, such as migraine, should be considered.
When a patient comes to Dr Archana Jhawar with persistent facial pain or headache, the ENT assessment begins with a detailed symptom history, what is the pattern, the triggers, what makes it better, what makes it worse, and what treatments have already been tried.
This is followed by nasal endoscopy, a thin telescope attach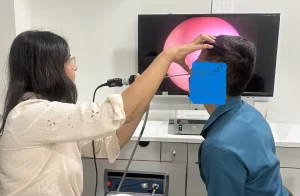 ed with high-definition camera) passed gently through the nose.
ed with high-definition camera) passed gently through the nose.
We can see inside of the nose like the condition of the nasal lining, the presence of any polyps or swelling, the degree of septal deviation, and whether there is any active infection or fungal debris.
You can see this in real time on the monitor.
This ENT consultation often provides more clinically useful information than a CT scan alone for a patient with chronic symptoms.
A true sinus headache is often accompanied by thick nasal discharge and a reduced or lost sense of smell.
If your headache includes sensitivity to light or sound, comes in episodic attacks, or occurs without any clear nasal blockage, migraine is more likely.
Sinusitis itself does not typically cause dizziness. If you have facial pain or pressure alongside dizziness or a floating sensation, vestibular migraine should be considered.
This is a distinct condition where dizziness and headache occur together as part of the same migraine process. An ENT specialist can assess both the sinus and vestibular components.
Bending forward shifts the pressure inside the sinus cavities, which worsens pain when sinuses are blocked or inflamed. This is a feature more typical of sinusitis than migraine.
However some migraine patients also find certain positions uncomfortable. It needs to be assessed alongside other features.
There are three common reasons. First, the headache may actually be migraine, which does not respond to antibiotics.
Second, the sinusitis may be viral or fungal, where antibiotics offer little benefit.
Third, structural problems such as nasal polyps or a deviated septum may impair drainage and require a different treatment approach.
Nasal endoscopy is generally well tolerated. A thin, high-definition endoscope is passed through the nostril after a brief decongestant preparation.
The procedure takes a few minutes. It provides real-time visual information about the nasal passages and sinus openings.
Dr. Archana Jhawar is a senior ENT specialist at Neoalta Clinic, Sector 17 Vashi with 25 years of experience in diagnosing and treating sinus conditions, nasal polyps, DNS, and vestibular migraine. Patients from Vashi, Koparkhairane, Kharghar, Nerul, Belapur and Panvel consult her for sinus evaluation and FESS surgery at Kokilaben Hospital, Koparkhairane.
See an ENT specialist if facial pain or headache keeps returning after antibiotics, if you have had more than two courses of antibiotics for the same symptoms, if your sense of smell is reduced, or if symptoms persist beyond 12 weeks.
These patterns suggest a structural, allergic, or non-sinusitis cause that will not resolve with repeated medication alone
Dr. Archana Jhawar, MS ENT with 25 years of experience, evaluates and treats sinus, allergy, vestibular migraine, and structural nasal conditions at Neoalta Clinic, Sector 17 Vashi and Kokilaben Hospital, Koparkhairane, Navi Mumbai.

Hi, I’m Dr. Archana Jhawar, an ENT specialist with over 24 years of experience. I specialize in tinnitus treatment, vertigo , ear care, and ear surgeries, practicing at Neoalta Clinic, Vashi, and Kokilaben Dhirubhai Ambani Hospital in Navi Mumbai. I’ve trained in vertigo management and Rational Emotive Behavior Therapy (REBT), combining science with compassion to offer holistic, evidence-based care. I’m passionate about writing, poetry, music, yoga, and photography.
Sinus Headache vs Migraine: How to Tell the Difference
Home Sleep Study vs Lab Sleep Study: Which One Do You Really Need?
Snoring, Gasping, or Fatigue: Is it Nasal Allergy or Sleep Apnea?
Nasal Allergy and Sleep Problems: Why You Feel Tired All Day